Fill a Valid DD 2870 Form
Simple PDF Forms
Fill a Valid DD 2870 Form
The DD 2870 form is often misunderstood. Here are nine common misconceptions about this form, along with clarifications to help clear up any confusion.
This form is applicable to both active-duty and retired military members, as well as their eligible family members. It is used to authorize the release of medical information.
While the form is primarily associated with medical records, it can also be used for other types of health-related information, including dental records and mental health evaluations.
The form is straightforward and designed to be user-friendly. Most individuals can complete it in a short amount of time.
A notary public signature is not necessary for this form. However, it must be signed by the individual granting authorization.
Currently, the DD 2870 must be submitted in paper format. Ensure that you send it to the appropriate office to avoid delays.
This form is valid only for a specific period, usually until the end of the treatment or for a designated timeframe. It’s important to renew it as needed.
While the individual must give authorization, a designated representative can request information on their behalf if specified in the form.
For certain situations, such as transferring medical records or obtaining information for legal purposes, this form may still be necessary.
Individuals can revoke their authorization at any time by submitting a written request to the relevant medical facility.
Understanding these misconceptions can help individuals navigate the use of the DD 2870 form more effectively.
Once you have the DD 2870 form in front of you, it's important to ensure that all sections are completed accurately. This form is essential for processing certain requests, so taking your time to fill it out correctly will help avoid delays. Follow these steps to complete the form effectively.
After completing the form, ensure that you keep a copy for your records. Then, submit it according to the instructions provided, whether that be by mail or electronically, depending on the requirements outlined for your specific request.
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is an important document for service members and their families. When filling out this form, individuals often encounter pitfalls that can lead to delays or complications in processing. One common mistake is failing to provide complete and accurate personal information. Missing or incorrect details, such as a Social Security number or date of birth, can hinder the ability of medical facilities to locate records or process requests.
Another frequent error involves not properly signing the form. The DD 2870 requires a signature from the individual authorizing the release of information. In some cases, people may overlook this requirement or mistakenly sign in a different capacity, such as a family member. This oversight can result in the form being rejected or returned for correction, causing unnecessary delays.
Additionally, individuals sometimes neglect to specify the exact information they wish to be disclosed. The form allows for the selection of particular medical or dental records. Failing to clearly indicate which records are needed can lead to confusion and may result in receiving information that is not relevant to the request. Clarity in this section is essential to ensure that the appropriate records are obtained.
Lastly, people often forget to review the instructions provided with the DD 2870 form. Each section of the form has specific guidelines that must be followed. Ignoring these instructions can lead to incomplete submissions or misunderstandings about the requirements. Taking the time to read and understand the guidelines can greatly improve the chances of a smooth and efficient processing experience.
| Fact Name | Description |
|---|---|
| Purpose | The DD 2870 form is used to authorize the release of medical information for military personnel and their dependents. |
| Who Can Use It | Active duty service members, veterans, and their family members can complete the DD 2870 form. |
| Submission Process | The completed form must be submitted to the appropriate medical facility or office that holds the records. |
| Confidentiality | Information released through the DD 2870 is protected under the Health Insurance Portability and Accountability Act (HIPAA). |
| State-Specific Laws | In addition to federal laws, each state may have specific regulations regarding the release of medical records. Check local laws for compliance. |
What is the DD 2870 form?
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is used by military personnel and their dependents. This form allows individuals to authorize the release of their medical or dental records to specific parties, such as healthcare providers or insurance companies.
Who needs to fill out the DD 2870 form?
Any military member or eligible dependent who wishes to share their medical or dental information with a third party must complete the DD 2870 form. This includes situations where medical records are required for treatment or insurance claims.
How do I obtain a DD 2870 form?
The DD 2870 form can be obtained through various sources. It is available online on the official Department of Defense (DoD) website or through military healthcare facilities. Additionally, individuals can request a copy from their healthcare provider.
What information is required on the DD 2870 form?
The form requires personal information such as the individual's name, Social Security number, and contact information. It also asks for details about the specific records being requested and the purpose for which they will be used.
Is there a deadline for submitting the DD 2870 form?
There is no specific deadline for submitting the DD 2870 form. However, it is advisable to submit it as soon as possible to avoid delays in obtaining the necessary medical or dental information.
Can I revoke the authorization after submitting the DD 2870 form?
Yes, individuals can revoke the authorization at any time. To do so, a written notice must be submitted to the party that received the authorization. It is important to specify that the revocation applies to the DD 2870 form.
What happens if I do not complete the DD 2870 form?
If the DD 2870 form is not completed, healthcare providers may not release the requested medical or dental information. This can lead to delays in treatment or issues with insurance claims.
Are there any fees associated with obtaining records using the DD 2870 form?
In most cases, there are no fees for obtaining medical or dental records through the DD 2870 form. However, some healthcare providers may charge for copying or mailing records. It is advisable to check with the specific provider for their policies.
Can I submit the DD 2870 form electronically?
Some military healthcare facilities may allow electronic submission of the DD 2870 form. It is best to confirm with the specific facility regarding their submission process. If electronic submission is not an option, the form can be printed and submitted in person or by mail.
Where do I send the completed DD 2870 form?
The completed DD 2870 form should be sent to the appropriate healthcare provider or facility that holds the medical or dental records. The specific address or submission instructions will typically be provided by the healthcare provider.
The DD 2870 form is essential for individuals seeking access to their military records. However, it often accompanies other forms and documents that facilitate the process. Understanding these additional documents can streamline your request and ensure you have everything you need.
Being familiar with these forms can enhance your understanding of the military records request process. Each document serves a specific purpose, and having them ready can save time and reduce frustration in obtaining the necessary information.
Progressive Insurance Logo Png - Features the Vehicle Identification Number (VIN) for identification purposes.
Odometer Statement Indiana - Odometer statements must be filled out completely to be considered valid.
The California Articles of Incorporation form is a legal document that establishes a corporation in the state of California. It outlines essential details about the company, including its name, purpose, address, and the names of its initial directors. For more detailed guidance on completing this important document, you can visit mypdfform.com/blank-california-articles-of-incorporation/. Understanding this form is crucial for anyone looking to start a business in California.
Bpo Template - Market statistics included in the form guide reasonable pricing adjustments based on local conditions.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
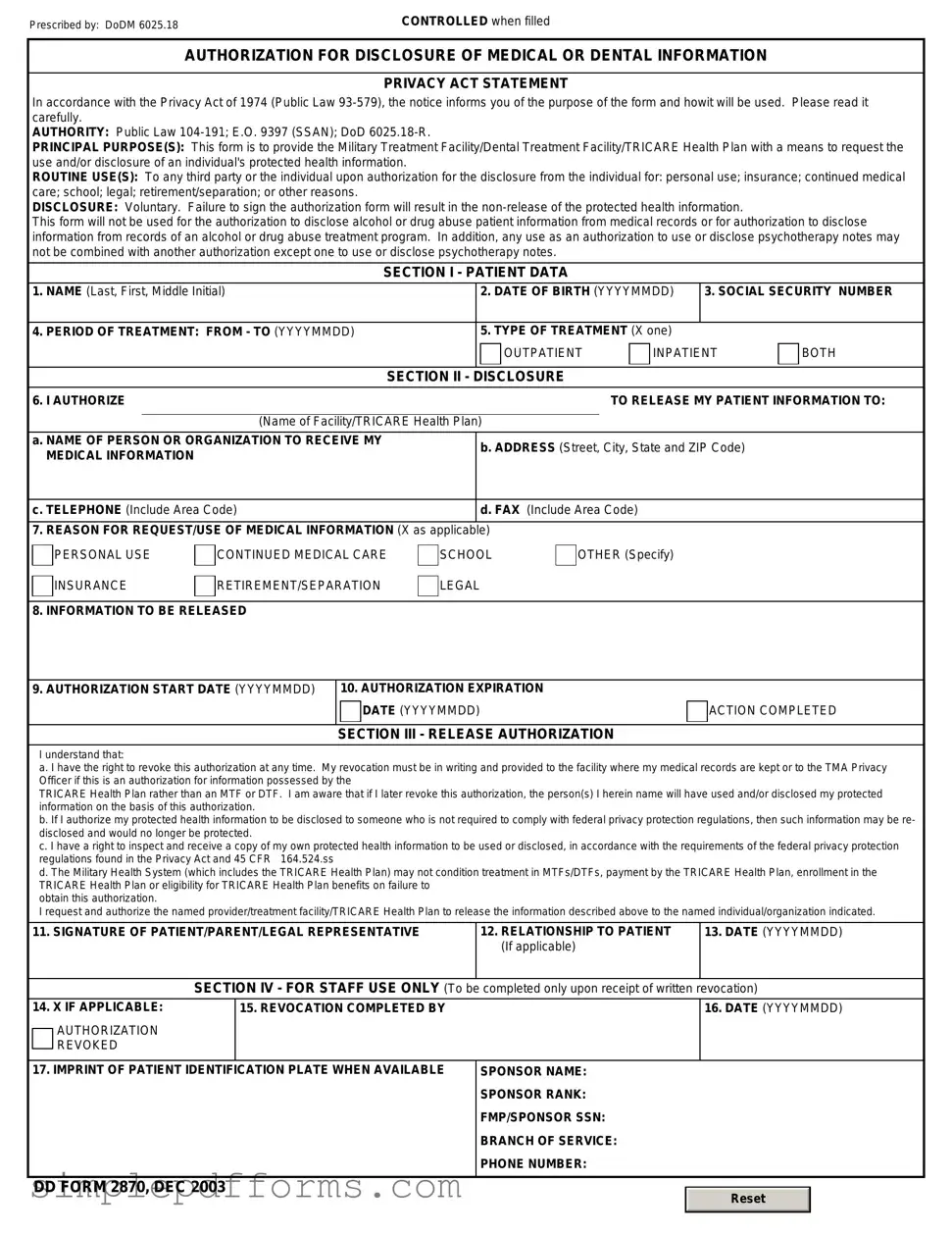
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|